
Today, the clinical landscape of IVF has achieved a significant milestone. For years, the integration of Artificial Intelligence was met with healthy scepticism regarding its “real-world” efficacy. However, as of this week, the first prospective randomised controlled trials (RCTs) have finally moved the needle from promising tech to a validated clinical partner. In today’s Science for Smile digest, we break down the landmark trial providing the evidentiary backbone for AI-supported selection in our daily practice.
Clinical Question
Does AI-supported embryo selection achieve non-inferiority to traditional morphological grading in a prospective, multicenter clinical environment?
The Mechanism: Beyond the “Beauty Shot”
Traditional grading is discrete and highly prone to intra- and inter-observer variability. The latest AI models, specifically Temporal Fusion Transformers (TFT), move past static, point-in-time assessments. By analysing over 7 million images from Time-Lapse Systems (TLS) and pairing them with 54 key clinical parameters (such as maternal age and specific stimulation protocols), the AI identifies “non-linear developmental trajectories.” It evaluates not just what the embryo looks like at a single moment, but how its unique kinetic rhythm predicts its future utilisation potential and chromosomal normality.
Evidence Summary: The Numbers You Need to Know
In a landmark RCT involving 444 patients across seven centres (validated May 14, 2026), AI-supported selection successfully met its primary endpoint for non-inferiority. The Clinical Pregnancy Rate (CPR) in the AI-supported arm reached 72.9%, compared to 68.0% in the traditional morphology arm. While the study is not yet statistically powered to claim superiority for live birth rates, the data demonstrate that AI provides a standardised, high-performance floor for selection. Furthermore, a recent meta-analysis of 20 studies confirms that AI models vastly outperform human capabilities, achieving a 81.5% median accuracy in predicting clinical pregnancy compared to the 51.0% median accuracy of solo human assessments.
The AI Workflow in Practice
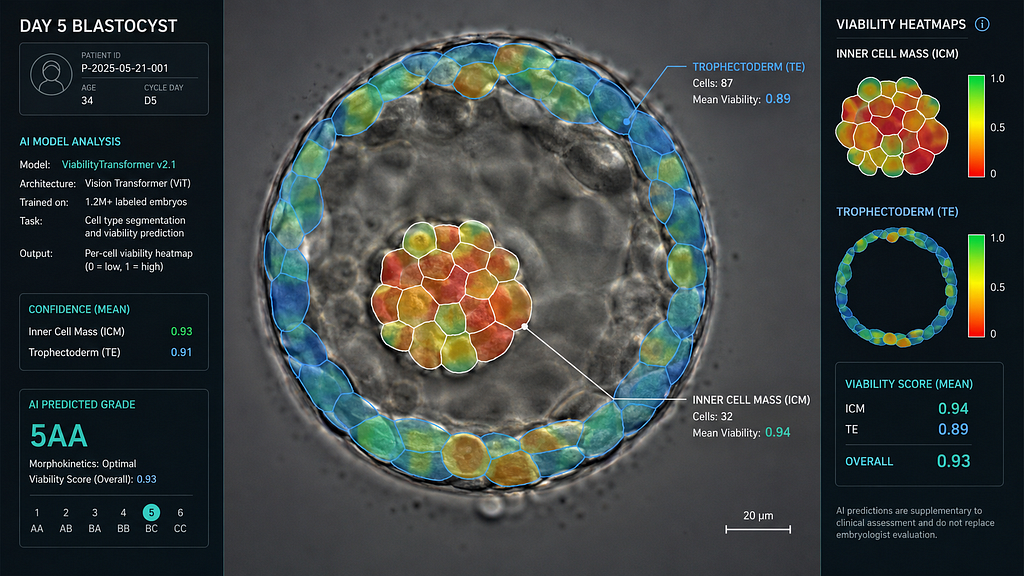
The clinical workflow operates as a seamless four-step pipeline. First, the system pulls the 3D-TLS video feed and automatically merges this Multimodal Input with the patient’s clinical history, including AMH, BMI, and protocol type. Next, the TFT algorithm performs Temporal Feature Fusion to identify critical “kinetic checkpoints,” such as the precise intervals from $t_5$ to $t_{SB}$. This powers the Predictive Scoring phase, where the AI generates a “Utilisation Score” predicting exactly when an embryo will reach a usable blastocyst stage. Finally, the workflow culminates in Specialist Oversight. The embryologist reviews the ranked cohort, and notably, clinicians successfully used their judgment to override the AI in 18% of cases, perfectly demonstrating the “AI + Human” synergy model.
Limitations & Clinical Bias
Despite these advances, a Predictive Ceiling remains a challenge for euploidy, with most models currently plateauing at an Area Under the Curve (AUC) of approximately 0.70. Additionally, there is a lack of widespread Generalizability Validation across diverse ethnic groups, specifically within the unique Indian demographic. To prevent Dataset Drift and ensure local accuracy, clinics must continuously feed localised datasets into these evolving models.
Practice Takeaway
AI is a standardizer, not a replacement. The data now firmly support AI as a safe, real-world clinical tool that reduces human error and administrative fatigue. For specialists handling high-volume cycles, implementing an AI-supported ranking system can help achieve a consistent >70% Clinical Pregnancy Rate. As an immediate next step for your clinic, begin integrating AI as a “Standardised Second Opinion” to minimise subjectivity during critical elective Single Embryo Transfer (eSET) decisions.
References
1. No One Had Proven If AI in IVF was complete BS. One RCT Just Changed That. Fertility Bridge / Alife Health, May 14, 2026.
2. Evaluating the concordance between AI-based and conventional embryo selection: a multicentre, retrospective, head-to-head analysis. PMC / RBMO, 2026.
3. AI is rewriting the rules of in vitro fertilisation: The Temporal Fusion Transformer. World Health Expo Insights, May 2026.
4. The potential, perils and pitfalls of Artificial Intelligence (AI) in Assisted Reproductive Technologies. PMC / NIH, March-May 2026.
For Clinicians: Stay at the forefront of reproductive science. Join our digital health collaborative to access real-time AI-driven benchmarks and advanced dose-prediction tools.
👉 Contact our Clinical Relations Team
https://www.google.com/search?q=https://www.santaan.in/contact-centres
Technical Metadata