
As we step into a fresh clinical week at Science for Smile, we are navigating away from pure downstream embryo selection to address the critical, often erratic launchpad of every IVF cycle: Controlled Ovarian Stimulation (COS).
For decades, gonadotropin dosing has remained an elegant guesstimate, a balancing act between maximising mature oocyte yield and mitigating the catastrophic risks of Ovarian Hyperstimulation Syndrome (OHSS). However, landmark multi-omic modelling data published this month in the Journal of Assisted Reproduction and Genetics (JARG) and Human Reproduction suggest that the era of empirical dosing is officially yielding to the “Digital Twin” framework.
The Clinical Question
Does an AI-driven, multi-parametric “Digital Twin” modelling framework provide a more accurate prediction of the Number of Oocytes Retrieved (NOR) and a lower incidence of cycle cancellation compared to standard AMH/BMI-based dosing nomograms?
The Mechanism
Traditional gonadotropin dosing relies on linear interpretations of baseline biomarkers, primarily Anti-Müllerian Hormone (AMH) and Antral Follicle Count (AFC). This method overlooks the intricate, non-linear physiology of multi-follicular recruitment.
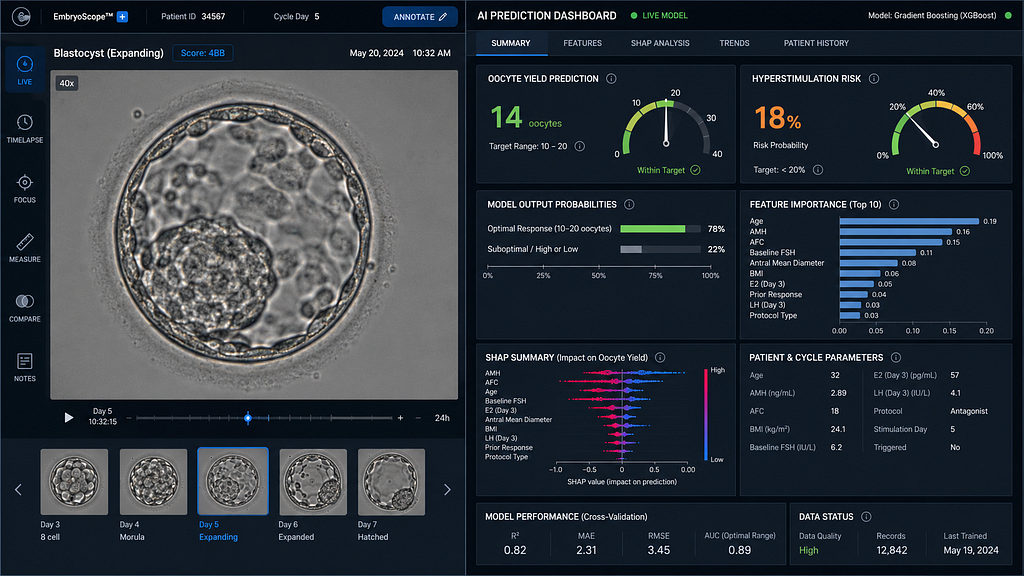
The advanced InOvaSGuide framework utilises a machine learning architecture powered by Gradient Boosting Regressors. By synthesising a patient’s multi-omic matrix, integrating age, BMI, baseline AMH, dynamic FSHR (FSH Receptor) polymorphisms, and baseline AFC, the algorithm constructs a virtual simulation, or “Digital Twin,” of the patient’s ovarian apparatus.
It then charts a personalised, multi-dimensional Dose-Response Curve. This allows clinicians to preview the exact point of diminishing returns: the threshold where increasing the gonadotropin dose ceases to yield more mature oocytes and instead exponentially drives up the statistical probability of VEGF-mediated hyperstimulation.
Evidence Summary
The clinical necessity of moving away from manual, calliper-based “cycle noise” was confirmed by a large-scale multicenter validation trial updated in May 2026.
- Predictive Precision: Across a diverse global cohort of 5,508 cycles, the AI-driven volumetric architecture achieved an R² value of 0.79 for predicting the precise number of oocytes retrieved. This represents a monumental leap in accuracy over traditional baseline nomograms.
- Follicular Precision: The underlying computer vision algorithm tracked follicles \ge 10\text{ mm} with a 98.2% precision rate, ensuring that true responders were never obscured by anatomical crowding.
- Workforce Efficiency: Automated follicular segmentation and predictive graphing reduced ultrasound probe-contact time by 66% and accelerated data annotation by 2.5x. This structural shift effectively mitigates clinician fatigue and standardises data collection across multiple branch clinics.
The AI Workflow
To conceptualise how this operates in a clinical setting, here is the breakdown of the platform’s architecture:
1. Multi-Dimensional Intake
Baseline clinical markers, demographic data, and genetic polymorphism variants are logged into the patient’s multi-omic profile within the clinical decision system.
2. Volumetric Sweep
The clinician performs a rapid 3D ultrasound. The system’s V-Net architecture segments the ovarian stroma and automatically maps the exact volume of the baseline antral pool.
3. Simulation & Optimisation
The Gradient Boosting Engine runs thousands of iterative simulations to plot the patient’s unique medication threshold and project their customised Dose-Response Curve.
4. Actionable Output
The Precision Trigger Dashboard generates a precise, individualised initial gonadotropin dosage and suggests an optimised “precision-triggering” window based on cohort synchronisation.
Limitations & Bias
The principal challenge for the Indian demographic remains “Phenotypic Drift.” Ovarian ageing and metabolic variations (such as insulin-resistant PCOS phenotypes prevalent across the Indian subcontinent) exhibit highly distinct, non-linear behaviours.
If the training data is predominantly skewed toward Western or East Asian biometrics, the algorithm’s predictive capability can face localised calibration errors. Continuous integration of domestic, multi-centre real-world data (RWD) is imperative to preserve model generalizability and safety.
Practice Takeaway
Does the Profile, Not the Protégé.
For high-volume practices where egg donors and complex hyper-responders are frequent, relying on conventional, static AMH cut-offs invites unnecessary cycle risk or sub-optimal yields. Embracing a “Digital Twin” model allows your clinical team to standardise the stimulation phase long before the patient steps into the retrieval suite.
By implementing automated volumetric tracking as a baseline protocol, clinics can safeguard patients from OHSS through data-led trigger timing, while systematically upgrading laboratory blastocyst conversion rates from day zero.
References
1. An artificial intelligence platform for automated measurement of ovarian follicles: a multicenter study. Journal of Assisted Reproduction and Genetics (JARG), 2026. PMID: [41485151].
2. Integrated Prediction System for Individualised Ovarian Stimulation and OHSS Prevention. Journal of Medical Internet Research (JMIR) / Reproductive Health, late Q1 2026 update. PMID: [41229699].
3. The problem with the ‘truth’: rethinking ground truth for artificial intelligence in reproductive diagnostics. Human Reproduction, Vol. 41, Issue 5, May 2026, Pages 650–657.
For Clinicians: Stay at the forefront of reproductive science. Join our digital health collaborative to access real-time AI-driven benchmarks and advanced dose-prediction tools.
👉 Contact our Clinical Relations Team
https://www.google.com/search?q=https://www.santaan.in/contact-centres
Technical Metadata