
Clinical Question
Does the use of AI-powered follicle counting and measurement software (FOLLISCAN) provide higher inter-operator reliability and accuracy in predicting oocyte yield compared to traditional manual 2D ultrasound monitoring?
The Mechanism
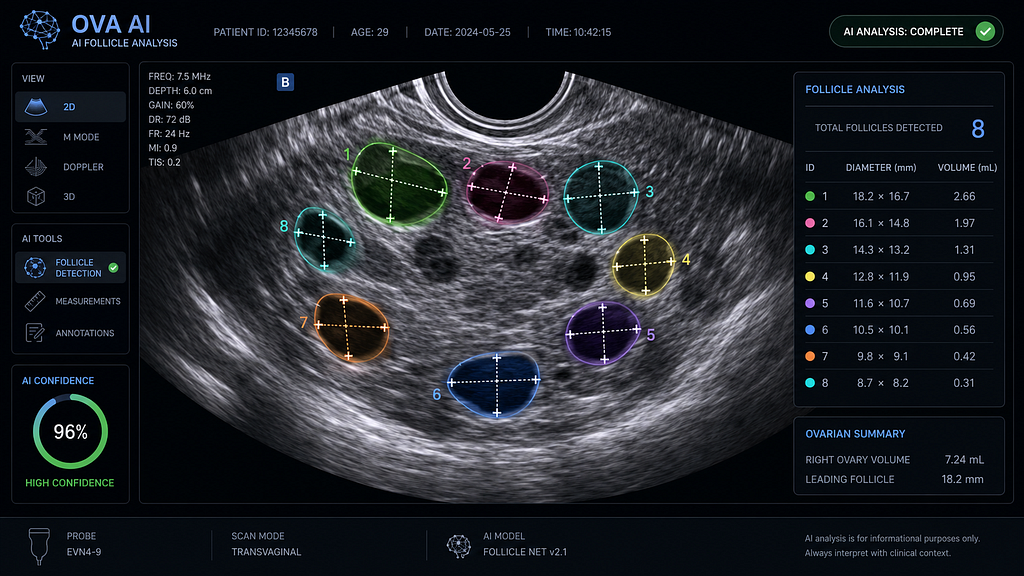
Manual follicular monitoring is notoriously prone to inter-observer variability, especially in high-responder cases where crowding makes individual measurement difficult. The FOLLISCAN AI framework utilises a 3D V-Net architecture (a variant of the U-Net used for volumetric data) to segment follicles from 3D ultrasound sweeps.
By calculating the Total Follicular Volume (TFV) and identifying the precise diameter of each follicle across three axes, the AI successfully mitigates the “geometric assumption” errors inherent in 2D manual measurements.
Evidence Summary
Evaluated across multiple Indian and European centres in the May 2026 issue of JARG, the AI-powered FOLLISCAN system demonstrated significant clinical advantages:
• High Accuracy: Achieved a 94.2% concordance rate with expert senior sonologists.
• Time Efficiency: Reduced the average monitoring time by 40% per patient.
• Superior Prediction: The AI’s “Follicular Growth Curve” proved to be a significantly better predictor of mature (MII) oocyte yield than manual diameter checks. This was particularly evident in patients with PCOS, where manual crowding often leads to under-counting.
AI Workflow
• Volume Acquisition: The clinician performs a rapid 3D ultrasound “sweep” of each ovary.
• Automated Segmentation: The V-Net algorithm identifies every fluid-filled structure, actively filtering out non-follicular artefacts like blood vessels.
• Real-Time Measurement: The AI calculates the mean diameter and volume for every follicle > 10 mm.
• Instant Reporting: A structured report is generated immediately, featuring a “Follicular Distribution Histogram” to assist the clinician in determining the optimal day for the hCG/GnRH-agonist trigger.
Limitations & Bias
The primary limitation is Artefact Interference. In ovaries with complex anatomy, such as those presenting with large endometriomas or internal scarring , the AI may occasionally misidentify cystic structures as follicles, resulting in false positives.
Additionally, the system relies on high-resolution 3D ultrasound probes. Because these probes are not yet standard in all tier-2 and tier-3 Indian clinics, there is a temporary “technology gap” in broader adoption.
Practice Takeaway
Efficiency is the precursor to Excellence.
In a busy IVF practice, manual follicle tracking is often the most significant administrative and clinical drain. Adopting automated monitoring does more than just save time; it standardises the trigger decision. This volumetric, granular view of the cohort significantly reduces the risks of premature triggers and Ovarian Hyperstimulation Syndrome (OHSS). As you prepare for your next high-volume clinic day, consider how automated tracking could enhance your oocyte yield through superior trigger timing.
References
1. FOLLISCAN AI for Ovarian Follicle Counting and Measurement Published in JARG. Journal of Assisted Reproduction and Genetics (JARG), May 2026.
2. A review of artificial intelligence applications in in vitro fertilisation: From follicular monitoring to pregnancy outcome prediction. PMC / NIH, May 2026.
3. Sperm DNA fragmentation: how to test, when to test, and what to do with abnormal results, a pragmatic mini-review for clinical practice. Human Reproduction, May 5, 2026.
For Clinicians: Stay at the forefront of reproductive science. Join our digital health collaborative to access real-time AI-driven benchmarks and advanced dose-prediction tools.
👉 Contact our Clinical Relations Team
https://www.google.com/search?q=https://www.santaan.in/contact-centres
Technical Metadata