
We are now moving beyond the “black box” phase of AI and into the first wave of prospective validation. Once seen as a promising newcomer, AI is now being tested against real-world outcomes. Emerging data from April 2026 is starting to define its true capabilities, highlighting where it surpasses the human eye, and where the embryologist still stands as the final arbiter of truth.
Ranking for Results: Moving from Morphological Subjectivity to AI Precision
Clinical question
Can AI-driven embryo selection achieve non-inferiority to traditional morphological grading in clinical pregnancy rates while reducing the time-to-conception?
Mechanism
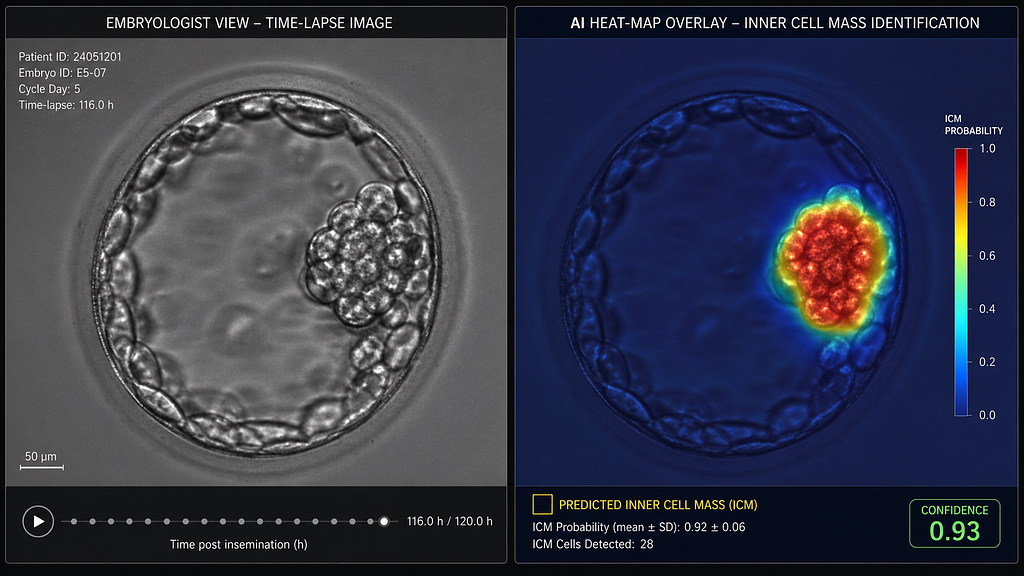
Traditional grading (Gardner criteria) is discrete and static. AI models, specifically Convolutional Neural Networks (CNNs), utilise “Feature Fusion”, combining pixel-level data from static images with kinetic data points from time-lapse imaging (TLI). By analysing non-linear variables such as the exact rate of trophectoderm expansion and the granularity of the inner cell mass, AI provides a continuous probability score (P) for implantation, rather than a categorical grade (e.g., 4AA).
Evidence summary
A landmark multicenter study published in Reproductive BioMedicine Online (RBMO) and updated in late April 2026 confirms that AI models are now achieving a 70.1% accuracy in identifying successful pregnancy outcomes, compared to an embryologist’s average of 67.7%. More importantly, a new prospective RCT involving 444 patients demonstrated that AI-supported selection is not only non-inferior to traditional methods but achieved a 72.9% clinical pregnancy rate in the AI arm versus 68.0% in the manual arm. While not yet statistically powered to claim “superiority” for live births, the data strongly suggest a significant reduction in “time to pregnancy” by ranking the most viable embryo first in the transfer order.
AI workflow
1. Standardised Capture: Blastocyst images are captured at exactly 110 \pm 2 hours post-insemination to ensure baseline consistency.
2. Segmentation: The AI isolates the blastocoel, trophectoderm, and zona pellucida, removing background noise from the culture dish.
3. *Deep Learning Analysis:* The model compares the current embryo against a dataset of >100,000 known-outcome embryos.
4. *Clinical Dashboard:* The specialist receives a “Viability Score” (0–10). If two embryos are graded “4AA” by the embryologist, the AI provides the tie-breaker based on sub-visual kinetic patterns.
Limitations/bias
The primary risk remains “Dataset Drift.” AI models trained on Caucasian or East Asian populations may not perfectly account for subtle physiological variations in the Indian population (e.g., differences in average BMI or ovarian reserve markers). Furthermore, AI cannot yet account for the “Uterine Factor” — it predicts embryo potential, not necessarily receptivity.
Practice takeaway
Standardisation is the new Gold Standard. Start by integrating AI as a “second reader” for your tie-breaker cases (where you have multiple high-grade embryos). This reduces the cognitive load on your embryology team and provides a data-backed rationale for patients when choosing which embryo to transfer first, potentially saving them the emotional and financial cost of an unsuccessful first transfer.
References
1. Evaluating the concordance between AI-based and conventional embryo selection: implications for clinical decision-making. RBMO, April 2026.
2. Multi-Centre RCT for AI-Assisted Embryo Selection Meets Study Endpoint. Fertility Bridge / Alife Health, March-April 2026.
Connect With Us
For Clinicians: Stay at the forefront of reproductive science. Join our digital health collaborative to access real-time AI-driven benchmarks and advanced dose-prediction tools.
👉 Contact our Clinical Relations Team
https://www.google.com/search?q=https://www.santaan.in/contact-centres
Technical Metadata